11/28/22-12/3/22
By Corrie Pelc on November 21, 2022 — Fact checked by Ferdinand Lali, Ph.D.
Dementia vaccines: What are they, and when could they become available?
Vaccines are arguably one of the greatest inventions of medical science of all time. Now, researchers are looking to take vaccine technology one step further to protect against neurodegenerative diseases like dementia. In this Special Feature, we asked experts about what is currently under development, how a dementia vaccine would work, and how quickly we may see one becoming available to the public.
Share on Pinterest
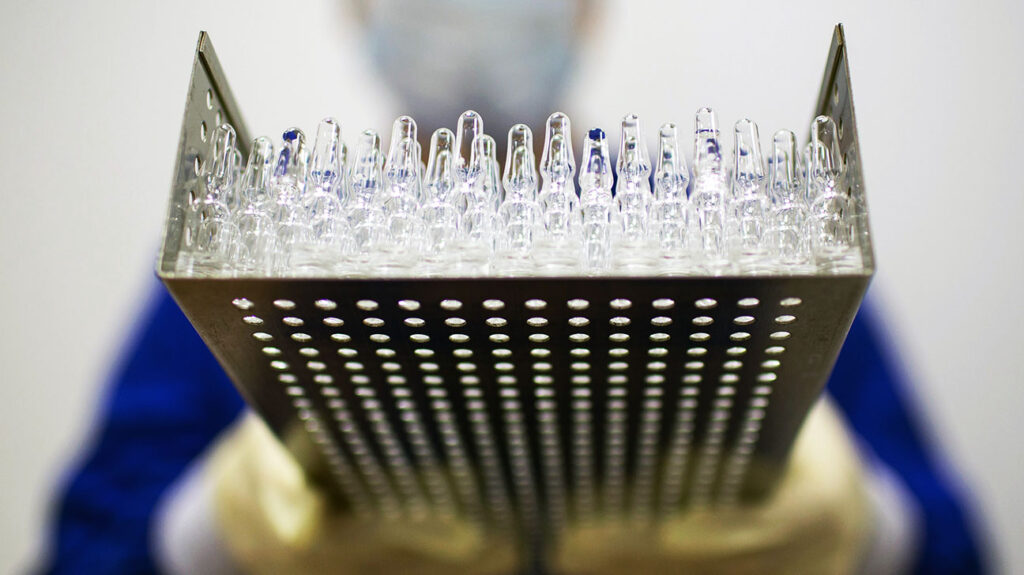
Will dementia vaccines ever become reality? We asked the experts. Image credit: Bloomberg Creative/Getty Images.
Dementia is an umbrella term referring to a range of disorders that affect the way in which a person’s brain works, causing symptoms including memory loss, behavior changes, and difficulty speaking
and walking.
The most common form of dementia is Alzheimer’s disease, which accounts for 60% to 80% of dementia cases.
More than 55 million
people around the world have dementia, with about 10 million cases added each year.
There are some Food and Drug Administration (FDA)-approved drugs for Alzheimer’s disease aimed at either changing disease progression or helping lower some symptoms of the condition. However, there is currently no cure for Alzheimer’s disease or most cases of dementia.
Is a dementia vaccine even possible?
Researchers are now looking at the possibility of protecting a person from developing dementia through a vaccine.
Traditional vaccines, such as vaccines for the flu and shingles, train the body’s immune system to fight off specific viral infections.
“More and more, there’s an appreciation of the immune system being relevant in the central nervous system, both in terms of driving a disease state, but also potentially recovering from or even preventing a disease from happening, including something as complex and devastating as dementia,” said Dr. David A. Merrill, a psychiatrist, and director of the Pacific Neuroscience Institute’s Pacific Brain Health Center at Providence Saint John’s Health Center in Santa Monica, CA.
He gave the example of recent evidence showing a person getting the flu or pneumonia vaccine might decrease their risk of developing dementia.
“It’s spurring the idea ‘could immune system activation or support actually help stave off the dementing process or nerve degenerative disease process?’,” Dr. Merrill continued.
“The starting point of the theories or hypotheses about Alzheimer’s didn’t start with ideas about the immune system, but it’s ending up that perhaps the treatments can and should involve helping or addressing immune system function with aging,” he told us.
What would a dementia vaccine do?
According to Dr. Michael G. Agadjanyan, vice president and professor of immunology at The Institute for Molecular Medicine in Huntington Beach, CA, vaccines against neurodegenerative disorders
are like subunit vaccines
— using only a piece of the pathogen — and recombinant vaccines
using DNA technology to raise antibodies against the most immunogenic peptide segments.
Dr. Heather Snyder, vice president of medical and scientific relations for the Alzheimer’s Association, said it is an exciting time in Alzheimer’s disease research, with over 100 potential therapies being tested at various stages of the research process, and many more being developed.
“There has been some research exploring active immunization, such as vaccines, to ‘protect’ individuals from Alzheimer’s,” she detailed. “These are vaccines that are being developed to target the biology related to Alzheimer’s.”
“They are, in some cases, leveraging the biology of decades of vaccine-related development more broadly in medical care. There are also different types of delivery systems and different types of biology that may be targeted with a vaccine for a potential therapy,” she explained.
Dr. Agadjanyan explained that dementia vaccines would generate immune responses against pathological molecules in the body associated with dementia, including:
-
proteins — toxic build-up of these proteins in the brain is often linked to Alzheimer’s disease
-
— a protein that helps stabilize the internal structure of neurons in the brain; abnormal tangles of tau protein in the brain are associated with Alzheimer’s disease
-
— a protein in neurons associated with Parkinson’s disease and Lewy body dementia when large amounts accumulate.
“In Alzheimer’s disease, the following processes develop in the brain tissues,” Dr. Agadjanyan explained to Medical News Today.
“[Beta-amyloid] plaques are formed from beta-amyloid protein. Inside the neurons of the brain, neurofibrillary tangles are formed from hyperphosphorylated tau protein. These accumulations of beta-amyloid and tau protein lead to the destruction of neurons and the development of inflammatory processes,” he said.
“As a result, neurons and the connections between them vanish, and memories, the ability to create them, and other human cognitive functions — thinking, the ability to concentrate on a task, logic, etc. — go with them,” he continued. “After a person receives a diagnosis of Alzheimer’s disease, they rarely manage to spend more than five to seven years in this world.”
Dr. Agadjanyan said that current scientific data suggest that aggregation of beta-amyloid is the critical feature for initiating Alzheimer’s disease followed by accumulation of pathological tau and, downstream, inflammation, oxidative stress, and neurodegeneration.
Dementia vaccines under development
A number of dementia vaccines are currently in different stages of clinical trials to study their effectiveness and safety, including:
-
a nasal Alzheimer’s disease vaccine from Brigham and Women’s Hospital in Boston entered the phase 1 clinical trial stage in November 2021
-
a phase 2 clinical trial is underway for Araclon Biotech’s Alzheimer’s disease vaccine targeting beta-amyloid 40
-
Swiss-based biopharmaceutical company AC Immune SA has a tau-targeted vaccine candidate for Alzheimer’s disease in a phase 1B/ 2A clinical trial.
Earlier this year, pharmaceutical company Vaxxinity announced it had received FDA fast-track designation
for its immunotherapeutic vaccine for Alzheimer’s disease. The vaccine candidate, UB-311, has completed phase 1 and 2A clinical trials, with phase 2B expected to begin in late 2022.
Dr. Snyder reported that the Alzheimer’s Association’s Part the Cloud program is currently funding an early-phase clinical trial testing the use of a vaccine in reducing brain inflammation in individuals with early Alzheimer’s disease. She stated that the trial is expected to finalize in fall 2023.
And Dr. Agadjanyan is part of a team at The Institute for Molecular Medicine (IMM) developing a vaccine
for Alzheimer’s disease.
“Our goal was to develop an immunogenic vaccine that can induce a sufficient level of antibodies in the periphery of all vaccinated cognitively unimpaired elderly with immunosenescence and delay/ halt the onset of Alzheimer’s disease,” he explained.
“We have developed a unique type of vaccine based on the universal platform technology MultiTEP, which we developed at IMM. This platform stimulates memory and naive T helper cells
, which in turn activate B cells
to produce antibodies at a much higher rate — up to 10 times — than vaccines currently used in clinical trials. With a large number of produced antibodies, the goal is to prevent/suppress the aggregation of [beta-amyloid] and/ or tau and stop or at least delay the onset of the disease.”
– Dr. Michael G. Agadjanyan
When will a dementia vaccine be available?
Dr. Merrill predicted it will be a while before any vaccines are available to the public.
“It’s still going to be a number of years before any vaccine is able to get through the development process, the regulatory hurdles, [and] the phases of clinical trials,” he pointed out.
Dr. Snyder agreed, and stated that the studies to date have been very small or in mice.
“More research in large, diverse human populations are needed before we can comment on the potential usefulness of a vaccine for protecting against or treating Alzheimer’s,” she advised.
Additionally, Dr. Merrill said people may be hesitant towards a dementia vaccine depending on how long the vaccination process may take.
“If you look at the early stage trials, the scheduling or the dosing of the vaccines can be quite variable,” he detailed. “In concept, you might hope for just a single dose vaccine and you would be protected, but the reality may be it might take a series. Monthly vaccination shots for a year is one design.”
“And the question is how interested will people be in getting this?” Dr. Merrill asked. “Clearly, if it truly protects and prevents you from getting Alzheimer’s, I think people would line up and would be very interested. But it’s all in the development of this — this is where it’s uncertain.”
Will dementia vaccines really work?
On the other side of the dementia vaccine argument is Dr. Karl Herrup, professor of neurobiology at the University of Pittsburgh School of Medicine.
He told MNT the dementia vaccines attempt to harness the power of the immune system to fight the biology of dementia and are all based on the hypothesis that deposits of misfolded proteins — amyloid, tau, and others — are the root causes of the disease.
“The vaccines, though differing in their strategies, are all based on using antibodies to the deposits to deplete and/ or remove them,” he explained.
“The bad news is that despite this biochemical success there is no meaningful clinical benefit to the therapies. Indeed in some trials, people on the drug actually fared worse than those on placebo. Many of us, myself included, have long argued that the hypothesis of aggregate-caused dementia rests on shaky grounds,” said Dr. Herrup.
“For us, the results were a bitter disappointment,” Dr. Herrup added. “I would rather be wrong and have a useful Alzheimer’s disease therapy than be right and have to have millions of people continue to suffer, but the results were not surprising.”
Dr. Herrup said that, in his opinion, the only important question about a dementia vaccine or treatment, for that matter, is whether the treatment slows or stops the clinical symptoms of the disease — cognitive decline and behavioral symptoms.
“I predict that none of these therapies will meaningfully alter the disease course,” he continued. “Sadly, since the industry poured most of its resources into these approaches, ignoring or sometimes repressing other avenues of investigation, it will be years before any meaningful therapies are available. For now, the best approaches are non-pharmacological.”
Share this article
By Corrie Pelc on November 21, 2022 — Fact checked by Ferdinand Lali, Ph.D.
Latest news
-
-
Almonds may improve appetite-regulating hormones, study shows
-
-
Feeling tired in the morning? 4 factors are key to alertness levels
-
-
Heart disease: Could your salt-shaking habits predict your risk?
-
-
Parkinson's: The distinctive shape of some proteins may aid early diagnosis
-
-
2 antioxidants found in dark leafy greens, tea linked to slower memory decline





Was this article helpful?
YesNo
In Conversation: New directions in dementia research
Millions of people around the world live with a form of dementia, which severely affects both their own and their carers’ quality of life. The specific causes behind dementia remain unclear, but researchers are making steady progress in finding out more about its mechanisms. This instalment of In Conversation looks at some of the realities of dementia, and presents new directions in dementia research.
Design by Andrew Nguyen.
Dementia is a neurocognitive syndrome that refers to a collection of symptoms related to memory loss and the decline of cognitive function.
The most common form of dementia is Alzheimer’s disease, which affects millions of people worldwide. According to data from the Centers for Disease Control and Prevention (CDC), in the United States alone, in 2020, as many as 5.8 million
people had Alzheimer’s disease.
Research conducted by the Alzheimer’s Society in 2019 indicates that over 850,000 people were living with dementia in the United Kingdom that year, and globally, more than 55 million
people live with dementia, according to the World Health Organization (WHO).
There are some treatments that can help alleviate some dementia symptoms, but most forms of dementia are currently incurable, and researchers continue to investigate the mechanisms through which this syndrome develops with a view to developing better treatments and prevention strategies.
In our latest instalment of In Conversation, we spoke with Paula Field, who is a caregiver for her mother who lives with Alzheimer’s disease, and with Dr. Kamar Ameen-Ali, who is a lecturer in biomedical science at Teesside University in the United Kingdom, and who specializes in neurodegenerative diseases, including Alzheimer’s.
This article provides an edited and shortened record of this instalment of our podcast. We have added reference links to key research findings mentioned in it. Please listen to the podcast — below or on your preferred platform — for the full discussion.
Dementia: Definition and genetic risk
Dr. Hilary Guite: Let’s start with an overview of dementia and its causes.
Dr. Kamar Ameen-Ali: I always think that it’s good when we are discussing dementia to start off with a definition of what we mean by it. Often you might hear people use it interchangeably with things like Alzheimer’s disease, but they’re very distinct things.
Dementia, we kind of describe it as an umbrella term. It describes a set of symptoms, it’s a clinical syndrome — those symptoms are often associated with memory impairment. But for a diagnosis of dementia, you also have to have an impairment in one or more other cognitive domains as well — this might be personality, it might be visual-spatial skills, for example.
And as I mentioned, dementia as a clinical syndrome is distinct from something like Alzheimer’s disease, which is a type of brain disease that leads to dementia.
Dr. Guite: Is dementia hereditary?
Dr. Ameen Ali: It depends on what brain disease we’re talking about. So if we’re going to talk about Alzheimer’s disease — which I think is a good idea, because it’s the most common brain disease that leads to dementia — there are some types of Alzheimer’s disease that are hereditary and some types that aren’t.
The most common type of Alzheimer’s disease is what we call sporadic Alzheimer’s disease, and that counts for 97% of Alzheimer’s disease cases. So 3% of cases of Alzheimer’s disease will have that known genetic origin, and this is caused by genetic mutations.
So only a small percentage of actual Alzheimer’s disease cases have got that genetic, known hereditary link.
The real-life impact
Dr. Guite: Thank you. So Paula, you’ve been looking after your mother with dementia alongside working. Can you tell us what you first noticed?
Paula Field: Yes, I am. I think my sister and I first noticed that there were some issues with her memory after my father had died. I think that she had started to develop some form of dementia before that, but [our parents] sort of helped each other out. And I think [our father] helped her through a lot of those daily things.
After he died, I think it became much more obvious [that something was wrong], but, you know, at that stage, we weren’t sure whether [her symptoms were] sort of a grief thing. But it gradually progressed. And it probably took us about 6 months or so after he died to realize that, you know, we probably did need to take her to the doctor, and to find out what was happening.
Dr. Maria Cohut: Paula, how did this affect you and your sister financially and during day to day life?
Paula: Well, I think in the early days, you could have a conversation [with our mother]. [My sister and I] were both working full-time, we’d go visit weekends, so we were there really regularly. In terms of financial impact, at that stage, there wasn’t very much, we just carried on as usual. We didn’t have any [additional] carers or anybody at that stage, we used to just go in as often as we could.
Then, once it got to the point when we had to take her to the doctors for her first memory test, and once the results came back, that’s when we had to start thinking about [arranging] more care. And that’s resulted in my sister having to take a day off a week from her work and spend two afternoons a week with my mom.
She has been doing that for nearly 4 years now. And we have other carers going in about twice a day now want to make sure that she gets up, and give her some lunch and the other one in the evenings, to give her some dinner. They do that about 4 days a week, and we pick up the rest.
How doctors diagnose dementias
Dr. Guite: What sorts of scans and diagnostic process happens nowadays?
Dr. Ameen-Ali: There are different types of scans that can be done, [such as] PET scans and MRI scans.
In terms of how well they can contribute to the diagnosis of brain diseases? Questionable, I think, because if we’re looking for brain changes that are associated with Alzheimer’s disease, for example, the question is how well can we see that pathology in the brain in life. Something like Alzheimer’s disease can actually only be diagnosed post mortem, when we can confirm that those pathological changes in the brain are actually there.
But something like a PET scan or a CT or an MRI scan, they can see whether there is that general atrophy in the brain, and that is something that we would expect to see in something like Alzheimer’s disease, particularly atrophy around the hippocampus, which is the part of the brain that is responsible for different memory processes.
So to a certain degree, these brain scans can help with the diagnosis of a certain brain disease that is leading to dementia, but we have to remember that it can only ever be confirmed post mortem.
Dr. Guite: You mentioned there atrophy, what does that mean?
Dr. Ameen-Ali: Atrophy is basically where the brain tissue degrades. If you were to see a brain that had atrophy, you’d see essentially shrinkage of certain areas of the brain.
Dr. Guite: My understanding is that the new PET scans can look at how the brain metabolizes nutrients, like sugar, and that they can show whether or not there are are some some proteins that get misfolded. Can you just explain what those proteins are — amyloid and tau — and how important they are?
Dr. Ameen-Ali: Amyloid and tau are the kind of characteristic pathological features of Alzheimer’s disease. Amyloid is a protein that will aggregate and clump together in the brain and form plaques, and that’s what we see in Alzheimer’s disease.
These plaques then disrupt neuronal cell function, and then that leads to a lot of those cognitive issues that we talked about earlier.
There’s also tau, which is [another] protein in the brain. Again, it’s another characteristic pathological feature of Alzheimer’s disease. Normally, it’s a protein within axons of nerve cells, and it helps to form what we call microtubules that are responsible for transporting nutrients within the cells.
What we see in Alzheimer’s disease, is that it aggregates into these tangles, and it disrupts cell function in that way, and it affects how cells communicate with one another.
Changes in personality and behavior
Dr. Guite: Paula, after that initial phase and the the memory loss, what else did you start to notice [in your mother]?
Paula: Well, we noticed that she became quite isolated. She didn’t leave the house, she did start to leave her peas on the cooker. And I think, you know, that was the point where we started to go, “Eek, this is getting quite serious.”
She still has some sort of instinctual habit, so she’ll still switch off the switches at the end of the day. That’s something that she’s done forever. But pretty much everything else…
She knows there’s a fridge in her house, and she knows that there should be something on the shelves, and she will put stuff in the fridge. It could be a packet of crisps or it could be a cup. She has this sort of visual memory of the fridge, she sort of knows what it’s for, but she doesn’t quite know how to use it.
But that’s about it. She doesn’t feed herself. If she won’t drink water, she certainly couldn’t take medicines. She does not wash [on her own]. If we ask her to wash her face or something, she’s quite canny, she’ll go in the bathroom, close the door, won’t let you in, and then come out again.
She still believes that she cooks her own dinner, she still believes that she can do all the things that she’s always done. I don’t think it’s denial, necessarily. I think she just [thinks that] it’s happened, therefore, she must have done it.
She has no idea who myself and my sister are — she recognizes us [as familiar faces], but she doesn’t know who we are. She has no knowledge of people going in every day to help her.
She’s not very active, she pretty much sits on her chair everyday with the TV on and looks into space.
Risk factors and what happens in the brain
Dr. Guite: Kam, can I come back to you from that devastating description of change in personality change in behavior, what’s actually happening in the brain? Because earlier you said [changes] started in the hippocampus, which is the area related to managing memories. But it sounds like more things are happening. What what would actually be happening as the dementia progresses?
Dr. Ameen-Ali: This is one of the complexities of these types of brain diseases that lead to dementia: First of all, how they can affect people very differently based upon the parts of the brain that are affected by the disease.
With something like Alzheimer’s disease, we we know that the pathology progresses into certain areas. And as the disease progresses, it starts to affect more areas of the brain, which is why you might initially see some memory problems.
But a lot of people might dismiss them as just getting older until then the disease progresses, and more and more cognitive domains start to be affected. So as the disease progresses to more of the cortical areas, you might see more issues around language around personality, and then visual-spatial issues that you might see later on as the disease progresses into those cortical areas.
Dr. Guite: Can we just look back to and understand why these things are happening? What are the risk factors related to chronic disease and exposures?
Dr. Ameen-Ali: If you remember, earlier on I mentioned sporadic Alzheimer’s disease — the Alzheimer’s disease that occurs in most cases. And it’s usually over the age of 65 that we would see that, so that when we’re talking about risk factors, they’re associated with that type of Alzheimer’s disease.
We have what we call non-modifiable risk factors. Those are those risk genes that I mentioned earlier on. Age and sex are also non-modifiable risk factors. Age is actually the biggest risk factor for something like Alzheimer’s disease.
But we also have these 12 modifiable risk factors. These are things that we do in our life that potentially we could change that can reduce our risk of dementia. And there are also, generally, things that we can do to promote good brain health, generally.
These modifiable risk factors include things like obesity, hypertension, diabetes, smoking, physical inactivity, loneliness… Brain injury is a big one as well.
Dr. Cohut: So some of the risk factors, but also the preventive interventions that get a lot of press are education and social activity. Presumably, the the longer you stay in education, and the more socially active and involved that you are the lower the risk of dementia. What about your mom, Paula? What was her experience of education and also social life?
Paula: Education minimal, if at all. You have to remember, she was born in the early ’30s. Her social social life was pretty good. [My parents] did have a group of friends when they were into their 50s–early 60s. They’d go on holidays together and and stuff like that. But that was quite sporadic.
And then they might see their friends every now and then. But predominantly, I would say they sort of stuck together. My dad was the social one, he had a much more active life.
Dr. Guite: How old was your mom when she left school?
Paula: Certainly no more than about 13. She wasn’t there very often. You’ve got to remember the [impact of the] war and evacuation and all that sort of stuff.
Dr. Guite: What is happening when we’ve got these elements of education, hearing impairment, social contact — how are they protecting against or reducing the incidence of dementia?
Dr. Ameen-Ali: These risk factors that we’ve talked about, we know that they’re associated with an increased risk of dementia. But what we’re trying to work out as scientists and as researchers is: What actually is the mechanism that is linking these risk factors with the kind of the disease that we see that then leads to dementia?
Because we can do studies where we can find out whether there is a significant correlation between these factors and dementia, but what exactly is causing something like brain injury to increase somebody’s risk significantly to then develop dementia?
The way that I like to imagine it is that our research into trying to understand these mechanisms is like the black box, that we’re trying to work out what’s happening inside that black box. So we’ve got these risk factors on one side, which is the input, and then the disease and the pathology, which is the output, but what is happening on the inside?
It’s almost like you’ve got risk factors and protective factors. And, you know, it’s all about that balance between minimizing your risk factors and maximizing the protective factors.
And it’s a game of probability, really, because there’s no guarantee that doing any of these things, you will get dementia. And there’s no guarantee that if you don’t do any of the things that you’ll be protected from it, but it’s all about managing risk, essentially.
Does neuroinflammation play a role?
Dr. Guite: I read that all of those 12 risk factors only account for 40% of dementia cases. So you’ve got the other 60%, which is in your black box. Can I come back to your black box now? Because we’ve got amyloid and tau, and we’ve got these risk factors, but what else is going on?
Dr. Ameen-Ali: Neuroinflammation is quite a significant area of research in terms of looking at a potential mechanism that would be driving brain diseases that lead to dementia.
Neuroinflammation is something that I’m interested in. There is a type of immune cell in the brain called microglia, and they’re involved in an inflammatory response in the brain.
A lot of the research that I’ve done is around brain injury. So I’ve looked at these cells, these microglial cells, and both the acute inflammatory response and also a chronic inflammatory response as a result of brain injury, and how that might be the mechanism that is increasing the risk of dementia after brain injury.
So it’s all about how the cells respond as part of a neuroinflammatory response in the brain. And how, over time, if there is a chronic response, because we know that neuroinflammatory responses are originally designed to be protective, but if it’s if the cells are activated long term, as in chronic activation, could they actually be causing damage? And could that be what is then leading to the development of the pathology that we see in something like Alzheimer’s?
Dr. Cohut: I was also thinking about some recent research that’s been looking at the gut-brain axis, so the link between the bacteria in our gut and what goes on in our brain. And there’s been some talk about the influence of gut bacteria on the brain in the context of dementia. So I’m wondering if that might have anything to do with neuroinflammation at any level?
Dr. Ameen-Ali: It’s possible, because when we’re talking about neuroinflammation, this could be systemic inflammation. It could be inflammation that’s happened at some point in a person’s life. It could be inflammation that has happened and then affected the brain.
So there is the possibility of inflammation that’s happened somewhere else in the blood, in the body that has then led to an inflammatory response in the brain. It doesn’t necessarily have to be from an injury that I look at in the brain, it can be systemic inflammation as well.
Early diagnosis is crucial
Dr. Guite: How are you feeling about the future for dementia and Alzheimer’s?
Paula: It’s a tricky one. I think, in our situation, if we’re to be brutally honest, it’s too late for any sort of treatment for my mom. For us, it’s just about keeping her safe, making sure she’s fed, making sure she drinks…
You know, my question is at what point do you think that people should approach their doctor for a diagnosis or a brain scan? Because, you know, in her case, we didn’t notice it, it was too late. I’m not saying they could have stopped it.
But at what point do you think that we need to get on top of this, and actually not wait until the diagnosis? Because once you’ve got a diagnosis, you know, there’s pretty little that you can do, and it’s sad, it’s a waiting game, and we don’t know what to expect. We had no warning, there was nothing that we could do about it in advance.
Dr. Ameen-Ali: I would say that [obtaining a] diagnosis as early as possible is the best thing to do, really. And that can be really challenging, because often, those early signs can be just dismissed as getting older or not really significant enough.
[However,] the earlier the diagnosis, the better, because [then] treatments will be the most effective. They can’t stop the disease, but they can have a much more significant impact on symptoms the earlier that they’re delivered.
I do think that going forward, we need to be able to diagnose much earlier, if we want to have effective treatments. And in terms of developing treatments, it’s unlikely that we’re going to have one single drug that is going to have a significant impact. Because there’s lots of these different potential disease mechanisms, it’s likely that we’re going to need different drugs that administered together, in parallel that will have any significant effect on disease progression.
Paula: Do you think that, potentially, we could get to a place where testing for or diagnosing dementia will be something like you’d have for breast cancer screening that becomes a routine part of your everyday medical self-care?
Dr. Ameen-Ali: I think so. I think if we have better cognitive tests that are more sensitive to certain types of memory decline, because different types of memory decline at different rates.
If we have sensitive tests, then we can certainly administer them at a certain age when your risk increases. And then hopefully that will start picking people up at an earlier rate when the disease is in its earliest stages. And that’s what I think will have a significant effect on on dementia in the future.
To discover more evidence-based information and resources for Alzheimer’s & dementia, visit our dedicated hub.
Share this article

By Maria Cohut, Ph.D. on June 28, 2022 — Fact checked by Catherine Carver, MPH
Latest news
-
-
Almonds may improve appetite-regulating hormones, study shows
-
-
Feeling tired in the morning? 4 factors are key to alertness levels
-
-
Heart disease: Could your salt-shaking habits predict your risk?
-
-
Parkinson's: The distinctive shape of some proteins may aid early diagnosis
-
-
2 antioxidants found in dark leafy greens, tea linked to slower memory decline





Was this article helpful?
YesNo
Alzheimer's study controversy: What does it mean for future research?
A now-seminal study published in 2006 provided evidence that the toxic accumulation of a protein called beta-amyloid in the brain was tied to the development of Alzheimer’s disease. Recently, an assistant professor from Vanderbilt University suggested that some of the images in this study were manipulated by the authors. What does all of this mean?
When a seminal Alzheimer’s study comes under fire, what are the ways forward? Image credit: Andriy Onufriyenko/Getty Images.
In 2006, a group of researchers from the University of Minnesota published a dementia-related study titled in the journal Nature
called “A specific amyloid-β [beta-amyloid] protein assembly in the brain impairs memory.” The study provides evidence supporting a specific protein clump in the brain, known as beta-amyloid
, as a cause for Alzheimer’s disease.
The study used a mouse model to show how these protein clumps — also known as amyloid plaques
— could cause dementia.
Because of its findings, this study became very influential in Alzheimer’s disease research. To date, it has been cited in over 2,200 scientific papers
and accessed more than 34,000 times.
Now an article recently published in Science reports that an assistant professor of neurology at Vanderbilt University believes some of the images were manipulated in the 2006 Nature study, calling into question the validity of its findings.
What is image manipulation in peer-reviewed articles?
is the process of changing a photograph. According to Dr. Elisabeth Bik, microbiome and science integrity consultant at Harbers-Bik LLC, photographic images can be easily digitally altered, for example, when we remove wrinkles or a mole from someone’s face in a photographic portrait.
“In scientific photography, you are not supposed to alter the image beyond some light general contrast adjustments applied to the whole image,” Dr. Bik explained for Medical News Today.
“Most journals nowadays explicitly forbid making any digital alterations. But if a researcher does an experiment, and the results are not as clean or if the results are completely different from what they expected, it is tempting and easy to digitally remove a stain or scratch in the background, or to add or remove some cells or change the thickness of a protein band. It is much faster to do some photoshopping than to redo the experiment.”
– Dr. Elisabeth Bik
This is certainly not the first time the images in a study have come into question. A study from 2016 — on which Dr. Bik was a co-author — found that 3.8% of scientific papers published in 40 journals between 1995 to 2014 had potentially problematic images, with at least half suggestive of deliberate manipulation.
To help fight the issue of image manipulation in scientific papers, in 2021, eight journal publishers outlined a three-tier approach
to help editors flag potentially problematic imagery.
What might this mean for dementia research?
MNT reached out to both Dr. Matthew Schrag, assistant professor of neurology and director of the Cerebral Amyloid Angiopathy Clinic at Vanderbilt University, who has made the allegations against the 2006 Nature study, and to the lead author of the study, Dr. Sylvain Lesné, associate professor in the department of neuroscience at the University of Minnesota. Neither of them responded to our questions.
A University of Minnesota public relations representative stated that the university is aware that questions have arisen regarding certain images used in peer-reviewed research publications authored by members of the University faculty, and that they were following due processes to review the questions any claims have raised.
Because of the influence that the 2006 Nature study has had on Alzheimer’s disease research, Dr. Bik said that if more research proves image manipulation, it would come as a blow to certain lines of enquiry.
“The 2006 Nature paper by Lesné et al. has been influential, and has led lots of researchers to pursue the same hypothesis and to replicate the study,” she pointed out.
“The AB*56 [beta-amyloid] work has also not yet directly led to any clinical trials. But it has encouraged several other lines of research that pursue slightly different angles, which have been tested in clinical trials. Yet, no experimental drug has been proven to be effective against Alzheimer’s,” added Dr. Bik.
“It is fair to say that the 2006 Nature study has led to a lot of wasted research money and effort, and raised a lot of false hope in patients,” Dr. Bik remarked. “There are other, alternative hypotheses to the beta-amyloid story, and perhaps there now will be more money to test those alternative ideas.”
Dr. Grace Stutzmann, professor and discipline chair of neuroscience and director of the Center for Neurodegenerative Disease and Therapeutics at Rosaline Franklin University of Medicine and Science, however, told MNT that even if the alleged image alterations in the 2006 Nature study were intentional, she did not think this would undermine all the research conducted in the field thus far.
“This case involves a specific single arrangement of beta-amyloid from a single lab that is in question, and there are many other amyloid variants that have been studied across multiple labs that were replicated,” she explained. “The [Alzheimer’s disease] field, in general, is much larger than just amyloid, so in reality, it’s a proverbial needle in a haystack.”
According to Dr. Sara Imarisio, head of research at Alzheimer’s Research UK, if these allegations of image manipulation are true, then, in the wake of the study, research groups may have planned experiments based on an erroneous premise, diverting valuable researcher time that could have been better spent elsewhere.
“But the findings from the paper were very specific and, contrary to some reports, have not significantly affected the progress or direction of research into Alzheimer’s,” she added. “Even for research groups who work in this particular area, findings that can’t be reproduced will be identified as controversial and lose credibility, while genuine findings will come to predominate and guide the direction of future studies.”
Dr. Maria C. Carrillo, chief science officer at Alzheimer’s Association, states that, as we continue to move forward, it is important to note that this investigation is related only to a small segment of Alzheimer’s and dementia research, and does not reflect the full body or science in the field.
“As such, this should not influence the field’s accelerating pursuit of the initial causes and other contributors to Alzheimer’s disease and other dementias,” she adds.
The Alzheimer Society of Canada also released an official statement regarding this matter, saying the allegations are a “serious concern and require deeper inquiry. Scientific integrity is crucial, and any potential diversion of money or time is a cause for concern.”
What can journals do to prevent future misconduct?
Dr. Charles Glabe, professor of molecular biology and biochemistry at the University of California Davis, stated that science depends on trust and the understanding that fabricators will ultimately be caught.
“Image duplication and copying were caught by software tools that compare bands on a gel pixel by pixel,” he noted. “This is good and well, but now that fabricators know that copying bands is easily caught, they will just run a different gel and use that one instead of publishing the same band twice.”
And Dr. John Hardy, professor in the Department of Neurodegenerative Diseases & Reta Lila Weston Laboratories at the UCL Queen Square Institute of Neurology, told MNT that it is very difficult to prevent fraud.
“One thing which has changed and was important in this case was image recognition software, which can catch stuff that previously people had got away with,” he said. “This has meant quite a lot of ‘old fraud’ has now been caught — like DNA testing of crime scenes.”
Moving forward, Dr. Bik said that to help scientific journals check for potential image manipulation there should be increased scrutiny by scientific publishers.
“Scientific publishers should spend some money and effort on quality control of submitted articles,” she advised. “They make a lot of profit but seem to not do enough screening manuscripts for signs of concern or fraud.”
“They should hire experts in statistics, ethics, and image forensics to screen such papers, and not rely on unpaid peer reviewers, who might not know how to look for misconduct.”
– Dr. Elisabeth Bik
“Journals and institutions should also penalize researchers proven to have committed misconduct, and be much quicker to retract papers,” Dr. Bik added. “Some of these concerns about the Lesné papers were already raised years ago. Journals and institutions are too slow and too hesitant to tackle these problems, and that will have to change.”
Share this article
By Corrie Pelc on August 2, 2022 — Fact checked by Alexandra Sanfins, Ph.D.
Latest news
-
-
Almonds may improve appetite-regulating hormones, study shows
-
-
Feeling tired in the morning? 4 factors are key to alertness levels
-
-
Heart disease: Could your salt-shaking habits predict your risk?
-
-
Parkinson's: The distinctive shape of some proteins may aid early diagnosis
-
-
2 antioxidants found in dark leafy greens, tea linked to slower memory decline





Was this article helpful?
YesNo
Medical myths: All about dementia
Welcome to the latest edition of our Medical Myths series. Today, to mark World Alzheimer’s Day, we will be tackling myths relating to both Alzheimer’s disease and dementia at large.

By Tim Newman on September 21, 2020 — Fact checked by Zia Sherrell, MPH
In our Medical Myths series, we approach medical misinformation head on. Using expert insight and peer reviewed research to wrestle fact from fiction, MNT brings clarity to the myth riddled world of health journalism.

Dementia is not a normal part of aging.
Today, an estimated 5.8 million
people aged 65 years or older in the United States have dementia.
Due to the fact that the average lifespan of people in the U.S. has increased over recent decades, some experts project that by 2050, the number of older adults with dementia could reach 13.8 million
.
Figures of this stature spark justifiable fear, and, as we have found in previous Medical Myths articles, fear tends to breed misconceptions.
In this article, we aim to dispel 11 of these myths.
1. Dementia is inevitable with age
This statement is not true. Dementia is not a normal part of aging.
According to a report that the Alzheimer’s Association published, Alzheimer’s disease, which is the most common form of dementia, affects 3% of people aged 65–74 years in the U.S.
As a result of the risk increasing as we age, 17% of people aged 75–84 years and 32% of people aged 85 years and older have a dementia diagnosis.
2. Dementia and Alzheimer’s disease are the same thing
This is not quite correct. Alzheimer’s is a type of dementia, accounting for 60–80% of all dementia cases. Other types of dementia include frontotemporal dementia (FTD), vascular dementia, mixed dementia, and Lewy body dementia.
The National Institute on Aging
define dementia as “the loss of cognitive functioning — thinking, remembering, and reasoning — and behavioral abilities to such an extent that it interferes with a person’s daily life and activities.”
Although dementias share certain characteristics, each type has a distinct underlying pathology.
Alzheimer’s disease is associated with a buildup of so-called plaques and tangles in the brain. These structures interfere with brain cells, eventually killing them. In contrast, brain cell death in vascular dementia occurs due to a lack of oxygen, which can result from a stroke, for instance.
FTD, as another example, occurs when abnormal protein structures form in the frontal and temporal lobes of the brain, causing the brain cells in these regions to die.
3. A family member has dementia, so I will get it
A common myth is that dementia is purely genetic. In other words, if a person’s family member has a dementia diagnosis, they are guaranteed to develop dementia later in life. This is not true.
Although there is a genetic component to some forms of dementia, the majority of cases do not have a strong genetic link.
As we learned above, rather than genetic factors, the most significant risk factor for dementia is age. However, if a parent or grandparent developed Alzheimer’s when they were younger than 65 years, the chance of it passing on genetically is higher.
Early-onset Alzheimer’s is relatively uncommon, though. It occurs in about 5.5%
of all Alzheimer’s cases.
As the majority of dementia cases are Alzheimer’s disease, this means that most dementia cases are not hereditary. FTD, which is much less common, has a stronger genetic link, but if a parent or grandparent develops the condition, it does not mean that children or grandchildren are guaranteed to develop it.
Today, FTD affects an estimated 15–22 in every 100,000
people. Of these individuals, 10–15% have a strong family history of the condition.
4. Dementia only affects older adults
Age is a risk factor for dementia, but dementia can affect younger adults in rare cases. Some scientists estimate
that, in people aged 30–64 years, 38–260 people in 100,000 — equivalent to 0.038–0.26% — develop early-onset dementia.
In the 55–64 age bracket, this increases to close to 420 people in 100,000, or 0.4%.
5. Using aluminum pans causes Alzheimer’s
In the 1960s, scientists injected rabbits with high levels of aluminum. They found that the animals developed neurological lesions similar to those that form in the brains of people with Alzheimer’s.
Additionally, some studies
have identified aluminum within the plaques associated with Alzheimer’s. However, aluminum also appears in the healthy brain, and researchers have not established a causal link between this element and the disease.
Following on from these studies, myths still circulate that drinking from aluminum cans or cooking with aluminum pots increases the risk of Alzheimer’s.
However, since those early experiments, scientists have not found a clear association between Alzheimer’s and using aluminum pots and pans.
Although researchers will, eventually, establish the precise relationship between aluminum and Alzheimer’s, consuming aluminum through the diet is unlikely to play a major role.
As the Alzheimer’s Society explain: “Aluminum in food and drink is in a form that is not easily absorbed into the body. Hence, the amount taken up is less than 1% of the amount present in food and drink. Most of the aluminum taken into the body is cleaned out by the kidneys.”
However, they also write that some research has found “a potential role for high dose aluminum in drinking water in progressing Alzheimer’s disease for people who already have the disease.”
6. Dementia signals the end of a meaningful life
Thankfully, this is not the case. Many people with a dementia diagnosis lead active, meaningful lives. Some people fear that if a doctor diagnoses them with dementia, they will no longer be able to go for a walk alone and will have to stop driving their vehicle immediately.
It is true that these adjustments may come in time as the condition progresses, but in mild cases of dementia, no changes
may be necessary. As dementia worsens, changes to the way an individual leads their life are likely, but that does not mean that the person cannot lead a fulfilling life.
“Too many people are in the dark about dementia — many feel that a dementia diagnosis means someone is immediately incapable of living a normal life, while myths and misunderstandings continue to contribute to the stigma and isolation that many people will feel,” explains Jeremy Hughes, former Chief Executive of the Alzheimer’s Society.
“[W]e want to reassure people that life doesn’t end when dementia begins.”
– Jeremy Hughes
7. Memory loss always signifies dementia
Although memory loss can be an early symptom of dementia, it does not necessarily signify the start of this condition. Human memory can be unpredictable, and we all forget things occasionally. However, if memory loss is interfering with everyday life, it is best to speak with a doctor.
Although memory issues tend to be an early sign

{kind=link}
{kind=link}
{kind=link}